Addiction Medicine
Avoiding stigmatizing language
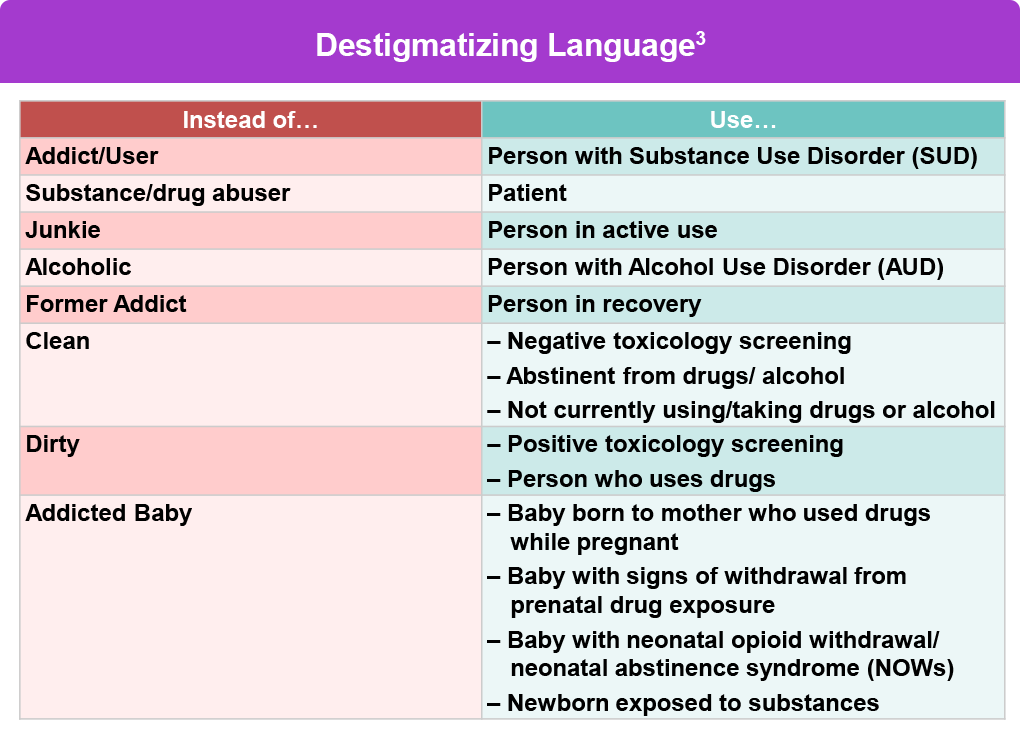
It is useful to look at the terminology around substance use disorders (SUDs), which can be stigmatizing and punishing.1 The language used can affect how willing people are in seeking necessary treatment. Stigmatizing language can also influence the HCP’s perception and care of the patient, as well as society’s perception of the individual with a SUD.1
Since HCPs are often the first-point-of-contact for people with a SUD, it’s important that they consciously assess the words and tone used while communicating.2 Certain words can promote bias and judgment towards people who have a SUD, for example the terms “abuse” and “addict”. Other judgmental language can be found around test results such as “clean” or “dirty”, where testing “positive” or “negative” is preferred.2
Differentiating addiction from tolerance
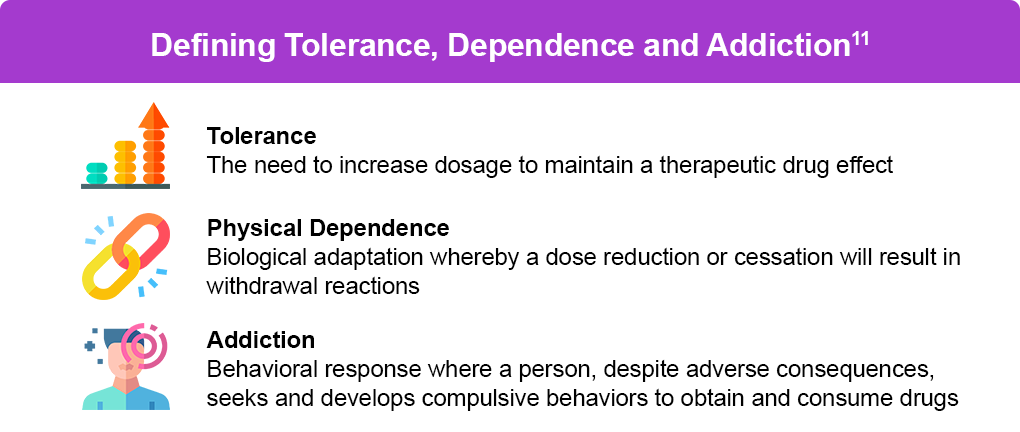
Tolerance is an important concept when discussing any drug, and is especially true for opioids.8 People who have been taking opioids for a while develop tolerance, where mechanisms in the brain respond less to opioid receptor activation, and more of the drug or higher doses are needed to produce the effect of pain relief.9 People who have recovered from an OUD are at greater risk for an overdose because they are unsure of the dose they can safely tolerate. As previously mentioned, tolerance and withdrawal are normal responses to long-term opioid use. However, addiction also involves a psychological component of craving and inability to control drug use. A cycle can develop when a person with an OUD experiences withdrawal, and uses opioids again to relieve these symptoms. Withdrawal symptoms can further exacerbate existing pain since it often involves severe bone and muscle aches, diarrhea, abdominal cramps, sweating, agitation, and anxiety.10 It is also possible to have OUD without physical dependence, and therefore does not experience symptoms of withdrawal or tolerance.11 This can happen if a person does not use opioids daily, but binges on them to the point of overdose.11
Treating opioid use disorder
References
- National Institutes of Health (NIH). Words matter – terms to use and avoid when talking about addiction. November 21, 2021. https://nida.nih.gov/nidamed-medical-health-professionals/health-professions-education/words-matter-terms-to-use-avoid-when-talking-about-addiction
- Johns Hopkins Medicine. Reducing the stigma of addiction. https://www.hopkinsmedicine.org/stigma-of-addiction
- Fagan B, et al. A multidisciplinary approach to treating patients with opioid use disorder in the primary care setting. 2024. https://serotarcnetwork.org/2024-opioid-use-disorder-symposium/
- US Food and Drug Administration (FDA). FDA Education Blueprint for Health Care Providers Involved in the Treatment and Monitoring of Patients with Pain. October2023. https://www.fda.gov/media/173774/download?attachment
- Ashford RD, et al. Biased labels: An experimental study of language and stigma among individuals in recovery and health professionals. Subst Use Misuse. 2019;54:1376-1384.
- Centers for Disease Control and Prevention (CDC). Preventing Opioid Use Disorder. May 8, 2024. https://www.cdc.gov/overdose-prevention/prevention/preventing-opioid-use-disorder.html
- Rasor J, Harris G. Using opioids for patients with moderate to severe pain. J Am Osteopath Assoc. 2007;107(9 suppl 5):ES4-ES10.
- Martyn JAJ, Mao J, Bittner EA. Opioid Tolerance in Critical Illness. N Engl J Med. 2019;380:365-378.
- National Institute on Drug Abuse (NIDA). Medications to Treat Opioid Use Disorder. October 2018. https://irp.nida.nih.gov/wp-content/uploads/2019/12/NIDA-Medications-to-treat-opioid-use-disorder_2018.pdf
- Wang SC, et al. Opioid addiction, genetic susceptibility, and medical treatments: A Review. Int J Mol Sci. 2019;20:4294.
- Lembke A. Tapering long-term opioid therapy. Am Fam Physician. 2020;101:49-52.
- Substance Abuse and Mental Health Services Administration (SAMHSA). Medications, counseling, and related conditions. Last updated March 28,2024. https://www.samhsa.gov/medications-substance-use-disorders/medications-counseling-related-conditions
- Bart G. Maintenance medication for opiate addiction: the foundation of recovery. J Addict Dis. 2012;31:207-225.
- Substance Abuse and Mental Health Services Administration (SAMHSA). Methadone. March 29, 2024. https://www.samhsa.gov/medications-substance-use-disorders/medications-counseling-related-conditions/methadone
- National Institute on Drug Abuse. What are misconceptions about maintenance treatment? May 2017. https://nida.nih.gov/publications/research-reports/medications-to-treat-opioid-addiction/what-are-misconceptions-about-maintenance-treatment
- Steve Rummler HOPE Network (SHRN). How MAT medications work. May 29, 2024. https://steverummlerhopenetwork.org/recovery/how-medications-work/
- Primary Care Providers Can Prescribe with Confidence. May 20, 2024. https://www.fda.gov/drugs/prescribe-confidence/primary-care-providers-can-prescribe-confidence
- Dydyk AM, Jain NK, Gupta M. Opioid use disorder. StatPearls. Last updated January 17, 2024. https://www.ncbi.nlm.nih.gov/books/NBK553166/
All URLs accessed September 11, 2024.
