Defining Pain
Persistent pain affects over 100 million Americans and contributes to over $600 billion dollars in indirect and direct healthcare costs in the US.1 In primary care offices, back, neck, headaches, and joint pain account for a majority of pain complaints. Globally, musculoskeletal pain the leading cause of disability.2,3 People seek pain management across a multitude of specialties and acuity settings, from emergency departments, surgical wards, podiatry clinics, and birth centers to dental offices, and long-term care facilities.4,5
Pain can also lead to a loss of productivity, and lowered quality of life.6 It can exacerbate or lead to other conditions, such as anxiety and depression, and can affect the well-being of family members and caregivers.7 It can also lead to a long-term dependence on analgesics, such as opioids. Untreated or inadequately treated pain can increase morbidity, prolong an injury or disease, and increase the cost of care.8,9
What is pain, exactly? In 2020, the International Association for the Study of Pain (IASP) defined pain as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage”.10 IASP adds a significant note that pain is always a subjective experience, and can vary through biological, psychological, and social influences.10 Pain can be acute, which can last a few seconds or up to days and weeks, subacute, lasting 6 weeks to 3 months, or chronic, which is any pain that lasts longer than 3 months.10,11 While subacute pain is a subset of acute pain representing ongoing healing, chronic pain itself can be a disease, called chronic primary pain, or indicative of an underlying disease or injury, where it’s called chronic secondary pain.3

The paradox of pain is that it is an important survival mechanism, protects the system from harm, and also helps to identify and avoid future harm from learned behavior.12,13 Pain can facilitate healing by allowing that area to rest by discouraging activity and overuse.14 Even though pain is a useful signal, it can greatly impact a person’s quality of life. Pain can also become maladaptive, sending continuous signals long after an injury has healed, or even in the absence of any disease or harm.15
Mechanisms of Pain
The mechanisms of pain can be understood by looking at three types of pain based on the damage that causes it. First, there is nociception, which is a process that responds to tissue damage through activity from receptors all over the body. It can be called the “detect and protect” system.16,17 The second type of pain is neuropathic, and occurs after disease or lesions to nerves. Unlike nociceptive pain, it has no protective function.16 The third type of pain is nociplastic pain, which occurs even though there is no evidence of tissue damage or evidence from disease or lesion of nerves in the somatosensory system.10
Nociceptive pain
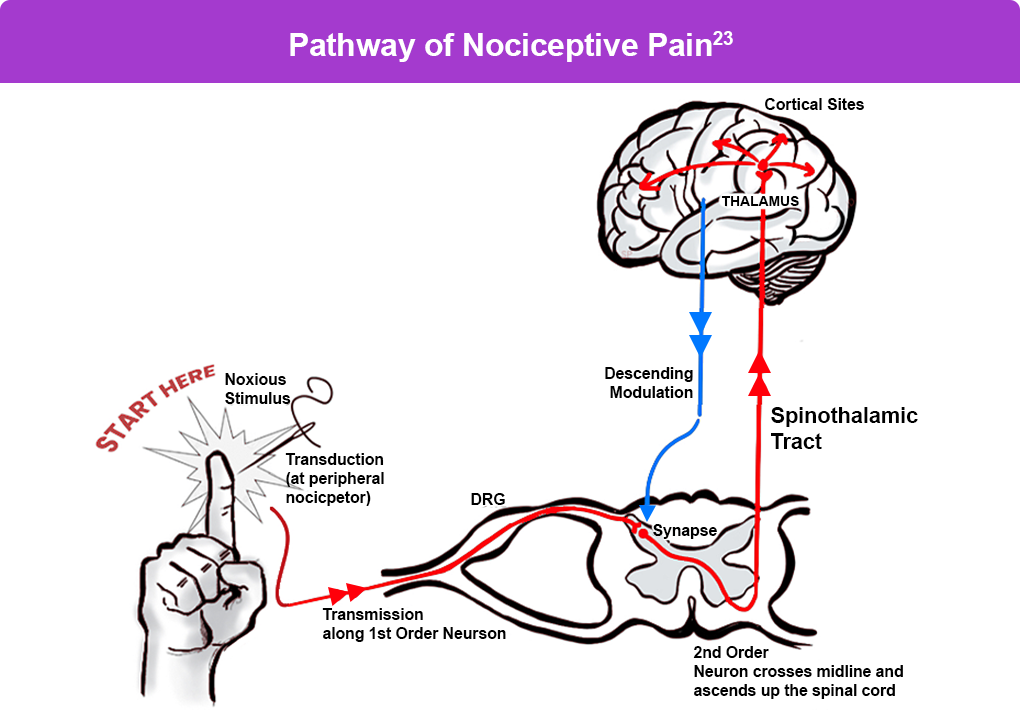
Nociceptive pain occurs when there is tissue damage from harmful or noxious stimuli. Receptors in bodily tissues and the nerve ending form a sensory unit called a nociceptor.21 Nociceptors are tuned to respond to external stimuli, such as injuries from a cut or a burn, or internal stimuli, such as chest or arm pain during a heart attack. Nociceptors can be subdivided into different types, for example cutaneous, visceral, muscle, and joint, among others.18 Nociceptive pain may also be chronic, as is in the case of osteoarthritis and inflammatory diseases.19
After nociceptors are activated, they trigger a pathway up the spinal cord into the brain. The thalamus area of the brain sorts the message and sends it to the sensory cortex which maps the area of the body where the sensation occurred.20,21 The experience of pain also depends on the interval or frequency between each action potential (or electrical impulses sending signals).18 As signals ascend up the spinal cord, there are also descending signals that contain pain-inhibiting chemicals, such as endorphins, serotonin, norepinephrine, and others.22
Neuropathic Pain
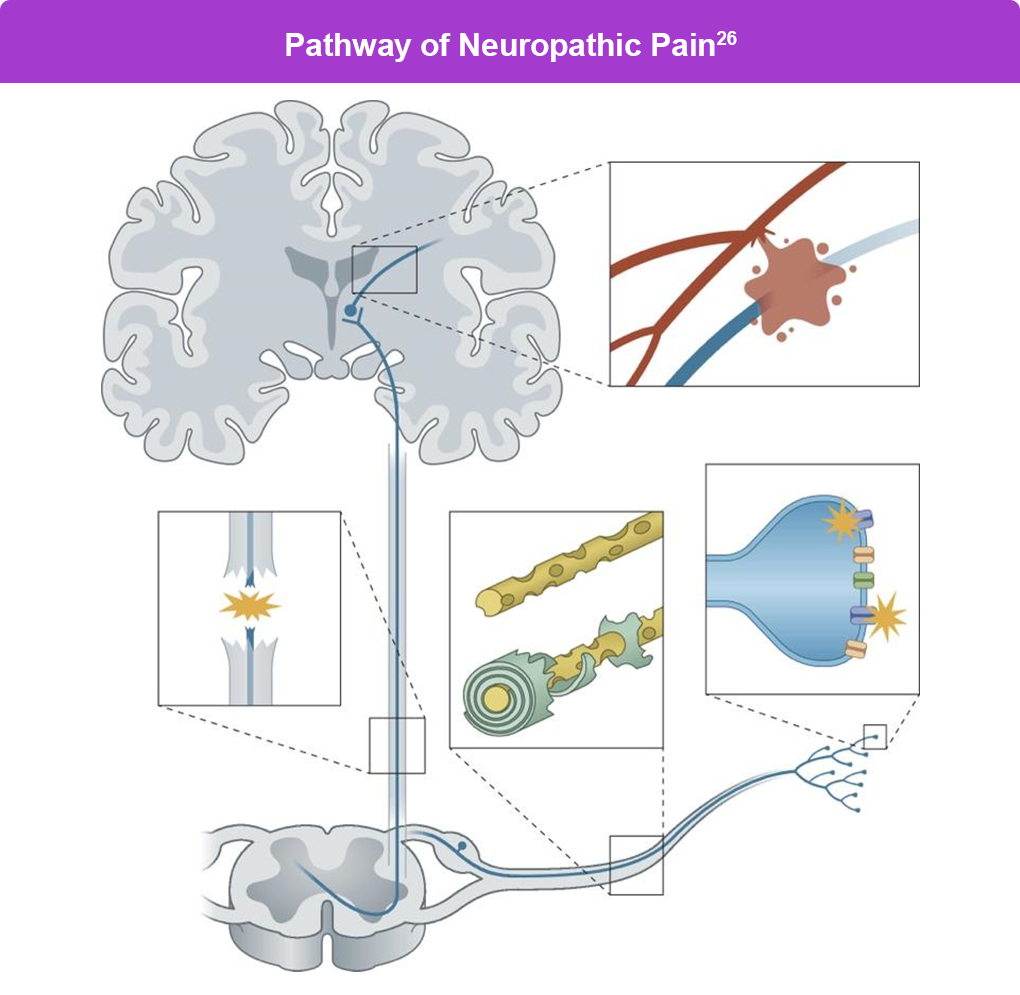
Neuropathic pain involves nociceptive pathways, and nociceptors nearby the damaged nerve can also contribute to pain.25 Examples of neuropathic pain include pain from diabetic neuropathy, multiple sclerosis, nerve compression, and phantom limb syndrome.20
Nociplastic Pain
A recently recognized pain category is nociplastic pain, which describes pain without identifiable tissue damage or lesion of the somatosensory system.10 Sensitization is the underlying mechanism of nociplastic pain.27 People can also have a combination of both nociplastic and nociceptive pain.10
In nociplastic pain, the pain may be more widespread and difficult to pinpoint, and can affect multiple areas of the body. Nociplastic pain can begin in a bottom-up approach similar to other types, but even minor pain or perceived pain is exaggerated. It can also be top-down, and can occur where there is no evidence of a pain trigger.28 Nociplastic pain recognizes that some chronic pain can be seen as diseases themselves, rather than symptoms of other diseases. The mechanisms of nociplastic pain are not as well understood, but there are similar alterations in pain pathways and augmentation in sensory processing systems as the other two types.29
Some argue that nociplastic pain is difficult to define and is challenging to discriminate from other types.30 There are discussions that a better distinction would be if the pain originates peripherally, or centrally (from the spinal cord or midbrain), although some pain can have both peripheral and central origins.29 Examples of nociplastic pain include chronic low back pain, fibromyalgia, and chronic fatigue syndrome.31
A newer term that is yet to be defined by IASP and other groups is “mixed pain”, a combination of all or some of the different pain types, and can be acute or chronic.32 Cases of mixed pain have been rising over the past 20 years, and include multiple chronic pain states, such as lower back pain, cancer pain, and osteoarthritis pain, among others. The mechanisms behind mixed pain are not yet well understood.32
Health-related quality of life (HRqol) is an important measure of how a disease or treatment affects a patient’s sense of overall function and wellbeing over time.33 It is a multidimensional assessment of physical, mental, and social health, and can be measured by through general scales, such as the Medical Outcomes Study 36-item Short-Form Health Survey (SF-36) or the condensed Short-Form 12 (SF-12) survey.34 There are also disease-specific scales, such as ones for arthritis that clinicians can choose from.33 HRqol in pain is increasingly used as a primary outcome in clinical trials, and is also a crucial measure for doctors to guide effective pain management and treatment.33
References
- Edwards RR, et al. Patient phenotyping in clinical trials of chronic pain treatments: IMMPACT recommendations. Pain. 2016;157:1851-1871.
- National Academies of Sciences, Engineering, and Medicine. Framing Opioid Prescribing Guidelines for Acute Pain: Developing the Evidence. The National Academies Press; 2020. https://nap.nationalacademies.org/catalog/25555/framing-opioid-prescribing-guidelines-for-acute-pain-developing-the-evidence
- International Association for the Study of Pain (IASP). Multidisciplinary Pain Center Development Manual. Chapter 1: The Need for Multidisciplinary Pain Centers. 2021. https://www.iasp-pain.org/resources/toolkits/pain-management-center/chapter1/
- Bowlby MA, Crawford ME. Opioid crisis and acute pain management after foot and ankle surgery. Clin Podiatr Med Surg. 2019;36:695-705.
- Ferrell BA. The management of pain in long-term care. Clin J Pain. 2004;20:240-243.
- Rikard SM, et al. Chronic pain among adults — United States, 2019–2021. MMWR Morb Mortal Wkly Rep. 2023;72:379-385.
- Yamaguchi M, et al. Insomnia and caregiver in chronic pain patients: A cross-sectional clinical study. PLoS One. 2020;15:e0230933.
- Chau K, Chau N. Association between untreated low back pain and injury proneness and confounding role of behavioral-health difficulties among younger adolescents: A population-based study. Eur Spine J. 2023;32:2069-2077.
- King NB, Fraser V. Untreated pain, narcotics regulation, and global health ideologies. PLoS Med. 2013;10:e1001411.
- International Association for the Study of Pain (IASP). Terminology. https://www.iasp-pain.org/resources/terminology
- Fenske JN, et al. Pain management. Michigan Medicine, University of Michigan; January 2021. https://www.ncbi.nlm.nih.gov/books/NBK572296/
- Di Maio G, et al. Mechanisms of transmission and processing of pain: A narrative review. Int J Environ Res Public Health. 2023;20:3064.
- Coll MP, et al. Pain reflects the informational value of nociceptive inputs. Pain. Published online May 7, 2024. https://journals.lww.com/pain/abstract/9900/pain_reflects_the_informational_value_of.595.aspx
- Nationwide Children’s Hospital. Understanding Pain. https://www.nationwidechildrens.org/specialties/comprehensive-pain-management-clinic/understanding-pain
- Price TJ, Dussor G. Evolution: The advantage of ‘maladaptive’ pain plasticity. Curr Biol. 2014;24:R384‑R386.
- St John Smith E. Advances in understanding nociception and neuropathic pain. J Neurol. 2018;265:231‑238.
- Woolf CJ. What is this thing called pain? J Clin Invest. 2010;120:3742-3744.
- Kendroud S, et al. Physiology, nociceptive pathways. StatPearls. Last update September 26, 2022. https://www.ncbi.nlm.nih.gov/books/NBK470255/
- Costigan M, et al. Neuropathic pain: A maladaptive response of the nervous system to damage. Annu Rev Neurosc 2009;32:1-32.
- Subedi B, Grossberg GT. Phantom limb pain: Mechanisms and treatment approaches. Pain Res Treat. 2011;2011:864605.
- Institute of Medicine (US) Committee on Pain, Disability, and Chronic Illness Behavior. Pain and Disability: Clinical, Behavioral, and Public Policy Perspectives. 1987. https://www.ncbi.nlm.nih.gov/books/NBK219247/
- Dubin AE, Patapoutian A. Nociceptors: The sensors of the pain pathway. J Clin Invest. 2010;120:3760‑3772.
- Center for Substance Abuse Treatment. Chronic Pain Management. Managing Chronic Pain in Adults With or in Recovery From Substance Use Disorders. Treatment Improvement Protocol (TIP) Series, No. 54. 2012. https://www.ncbi.nlm.nih.gov/books/NBK92054/
- Parikh AA, et al. Pain and Placebo Physiology. PM&R knowledgeNow. Last updated December 15, 2020. https://now.aapmr.org/pain-and-placebo-physiology/
- Campbell JN, Meyer RA. Mechanisms of neuropathic pain. Neuron. 2006;52:77-92.
- Finnerup NB, Kuner R, Staehelin Jensen T. Neuropathic pain: From mechanisms to treatment. Physiol Rev. 2021;101:259-301.
- Nijs J, et al. Nociplastic pain criteria or recognition of central sensitization? Pain phenotyping in the past, present and future. J Clin Med. 2021;10:3203.
- Fitzcharles MA, et al. Nociplastic pain: Towards an understanding of prevalent pain conditions. Lancet. 2021;397:2098-2110.
- Loeser JD. A new way of thinking about pains. Pain. 2022;163:1670-1674.
- Fernández-de-Las-Peñas C, et al. Myofascial pain syndrome: A nociceptive condition comorbid with neuropathic or nociplastic pain. Life (Basel). 2023;13:694.
- Bułdyś K, et al. What do we know about nociplastic pain? Healthcare (Basel). 2023;11:1794.
- Trouvin AP, Perrot S. New concepts of pain. Best Pract Res Clin Rheumatol. 2019;33:101415.
- Sitlinger A, Zafar SY. Health-related quality of life: The impact on morbidity and mortality. Surg Oncol Clin N Am. 2018;27:675-684.
- Huo T, et al. Assessing the reliability of the short form 12 (SF-12) health survey in adults with mental health conditions: A report from the wellness incentive and navigation (WIN) study. Health Qual Life Outcomes. 2018;13;16:34.
All URLs accessed September 11, 2025.
